Strategy 8 -- A simple but effective momentum futures trading strategy
We are trading futures (micros) again. This one made $52K in the last 4 years with 1155 trades and a 78% win rate. PF 1.4, Sharpe 1.4, RoR 9.7%, MaxDD 6%


Disclaimer: the following post is an organized representation of my research and project notes. It doesn’t represent any type of advice, financial or otherwise. Its purpose is to be informative and educational. Backtest results are based on historical data, not real-time data. There is no guarantee that these hypothetical results will continue in the future. Day trading is extremely risky, and I do not suggest running any of these strategies live.
While I was creating Strategy 7, which is a simple mean reversion strategy, I made a joke in a chat about creating a momentum strategy that used the same entry signals as Strategy 7 but in reverse. I didn't really intend to actually test the idea out until I was looking at some of the trade charts from 7.
Strategy 7 works, as a mean reversion strategy, but it also utilizes volatility adjusted limit order to place trades. That means it can place a short trade on a historically green bar and still be profitable. However, those bars on the chart were green, not red. So, if you just long the short signal at the open, it should result in a winning trade. Right?
That's where this idea started, anyway. I decided to script it just to see if worked exactly as it was, and it did, but not well. A few pivots later, I found Strategy 8, hiding in what began as a strategy that would probably never get posted. I thought about scraping the idea and moving on to the next one, but something about it kept tugging at me, so I kept pivoting until I found what I was looking for.
In the end, the strategy is actually simpler than its predecessor. I have always been a fan of simple techniques. Simple techniques are easier to practice and easier to master. This was rule that held true in EMS as well...
This is a long one. Feel free to skip it if you have access to the strategy portion of the post. Also, medical procedures that were conducted on a trauma patient are discussed. If that isn't something you are into, that's okay too. You can become a paid subscriber and skip straight to the strategy details. Don't forget to check out the backtest results on the way.
Lessons from the Past
Working during a holiday in EMS is always a bit of a crap shoot, and Christmas is no exception. They are typically slower, but not always. The people who do call in on Christmas tend to be more likely to actually be having a medical emergency. One of the last Christmases I worked was a few years back when I was at a rural county fire department in Georgia. I was technically a new hire and still performing my "third-rides." This is when an employee works as a third person on the ambulance until the medic signs off on them to work by themselves or they meet whatever requirements the department has.
This was likely going to be my last third-ride before going to my own truck, and my FTO for the day was a young paramedic who had been licensed as a medic for maybe 1-2 years. I had just returned home from contracting overseas that year and was closing in on the end of my 9th year in EMS. The amount of experience the third-rider has doesn't usually matter. It's a process.
On this Christmas day, it shouldn't have mattered either. However, instead of the slow, no-call shift we were hoping for, we ended up with three calls. It takes an hour just to get to the hospital from the county we worked in, so calls tend to be on the long side.
The original plan was just to have me drive the whole day so I could learn the roads—something I actually needed to practice. No one likes a medic or EMT who doesn't know their way around. Firefighters drill this kind of thing, but not so much in EMS. I was working at a fire department, so knowing my way around would be a big benefit.
Instead, what we got were three calls, and every one of them required I stay in the back with the patient and my FTO and help manage the patient. The first two calls were medical, and both patients were treated and transported. The third call was to a single-vehicle accident on a dirt road.
You go to these calls trying to game it. It doesn't matter how long you've been doing it. It's in our nature to try and game the scene before we get to it. As long as you know how to pivot when you are wrong, it's okay.
How bad could a single-vehicle car accident on a dirt road be on Christmas day?
The first pivot happened when we got on scene and realized we needed to put our game faces on. The car looked like it struck a tree at an incredible rate of speed. To help you visualize the damage, the floorboard of the car was gone like it was a Flintstone car. It was still on the wheels, thankfully. Oh yeah, it happened in front of the driver's home, so their family was on scene screaming at us for responding too slowly. In her defense, no units were close to the call, from what I recall.
The next pivot happened when we realized there were two patients on scene: one ejected and one in the car. Luckily, we had two ambulances respond, and we arrived around the same time. We got the vehicle extrication and patient, they got the ejected patient. This was decided on the move and probably not even talked about out loud.
Vehicle extrication isn't an exact science, but there are some foundational concepts that can help you along the way should confusion, exhaustion, or Murphy alter the way you always practice. When we got to the car, two things were clear: the patient in the vehicle was in critical condition, and the patient needed out of the vehicle as quickly as possible and en route to the trauma center. The only thing standing in the way was a crumpled door from a massive bend in the car's frame.
This is the part of the job that the more firefighter-oriented types love. They love their hydraulic tools, too. Working overseas, we used to practice vehicle extrication every chance we got. We used up-armored Chevrolets, Toyotas, and BMWs. Armor doesn't care about your fancy tool. It won't bend. You have to really focus on those foundational concepts. Expose the door latch mechanism and force it open. The only other option is the windshield, which you would have to remove as a single unit, due to it being several inches thick and rated to withstand several high-powered rifle rounds. We had some electric-powered hydraulic tools, but they were a luxury. We practiced a lot with the good ol' sledgehammer, a Halligan tool, and a pair of bolt cutters if necessary.
Back to our accident scene, and my partner is working on the door with a hydraulic spreader while I assess the patient’s condition (it isn’t good). Except, the spreader is failing and won't generate the force needed to pop the door by force (which can't be done on an armored vehicle). The first thing that came to my mind, briefly, as I had my hands full too, was to expose the latch and snap it with bolt cutters.
But I never had to say it. My young partner made the next pivot without having to discuss it. Soon enough, the door was open, and we extricated our patient without spending an extra minute on scene. When we got to the ambulance, our Lieutenant had already pulled all the medications he anticipated we would need for our patient. It wasn't too hard. He was dying. He assisted us in getting the patient ready for transport, we thanked him for his service, kindly asked him to leave, and beat it to the hospital. In the end, the patient needed a surgeon, not a paramedic.
Managing a multi-system trauma patient is not an easy task, whether you are in the hospital or not, have one or two medics in the back or an endless supply of minions. Medications and gadgets and hands help, but there are a lot of things that have to go right, and the patient can't be allowed to code (cardiac arrest), or the likelihood of survivability takes a massive shit. There is also a lot riding on the fight in the patient. Can't forget about that.
Our patient was rapidly sedated and intubated. My partner started here (while I gave meds) but turned it over to me when he couldn't visualize the cords with the camera-assisted blade or they were clamped shut. I used a Mac 3 and a bougie, waited for him to take one of his gasping, random breaths, and sent it home. An old-school technique nowadays. After a few minutes, and things calmed down a little bit, the patient became difficult to bag, lung sounds were muffled, and SPO2 was starting to decline. We had a pneumothorax, possibly bilateral.
Any medical drama fans here? You know what I'm talking about.
The final pivot: my partner had never done a needle decompression (ND) on a patient before. Lucky me, because the patient needed two, and this was a perfect learning moment. I walked my partner through the ND on his side of the patient.
Too easy. I moved to my side and... what the fuck?
The ND goes under your arm (anterior axillary line) and into your side. It is designed to relieve pressure on the chest cavity caused by air buildup. It can happen without trauma, but it isn't uncommon in massive trauma events. Well, I couldn't find the site for the procedure on my side. There was something wrong with his ribs (a flail chest). I pivoted to the second site (on the upper chest, midclavicular) and walked through the procedure again.
Back to the Present
The patient made it to the hospital with pulses intact. He then made it through everything else that came after and last I checked was recovering well. Things don't always go as planned, and they don't always happen the way you practiced it. In this scenario, I had a lot of practice on trauma scenarios and I leaned heavily on basic techniques that work and that I had practiced over a thousand times.
Once you learn the basics, and practice them religiously, the pivot becomes the art. How you piece together the things you learn when you need them. I have found the process of researching trade strategies and ideas to be very similar. I start with one idea, and by the end of it, I have something that looks very different than what I jotted down in my notebook.
That's how Strategy 8 went. I started with the reversed signals, and then slowly took it apart and pieced it back together with the same techniques that I have been working on and improving. When I was done, it was its own momentum strategy that had decent results. Instead of scraping it, or giving up, I just kept pivoting until it had shape that wasn't over fit or overly complicated.
That paramedic eventually become my partner and, since I haven't been back to EMS since working there, was the last person I worked EMS with. Good times. Now, let's see if we can keep it that way.
Backtest Results
Start Date: 01-02-2020
End Date: 07-011-2024
Data Series: Daily
Universe: Equity futures contracts. ES/MES, NQ/MNQ, YM/MYM, RTY/M2K, and EMD
Side: Long
Type: Momentum
Strategy Stats

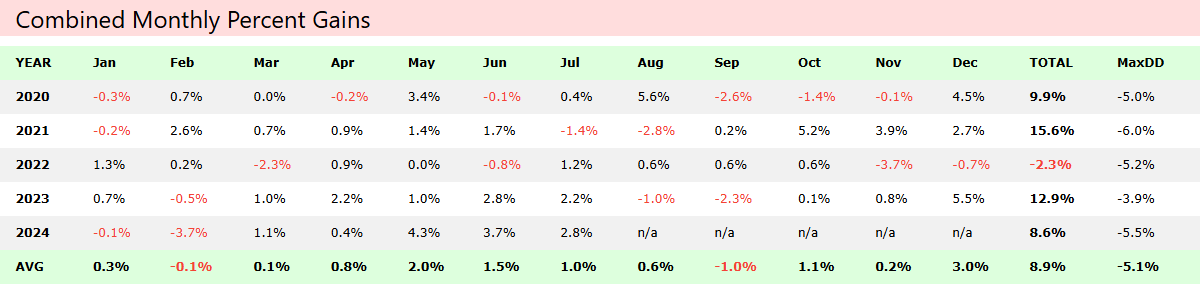
Combined Monthly Percent Gains
Equity

Drawdown

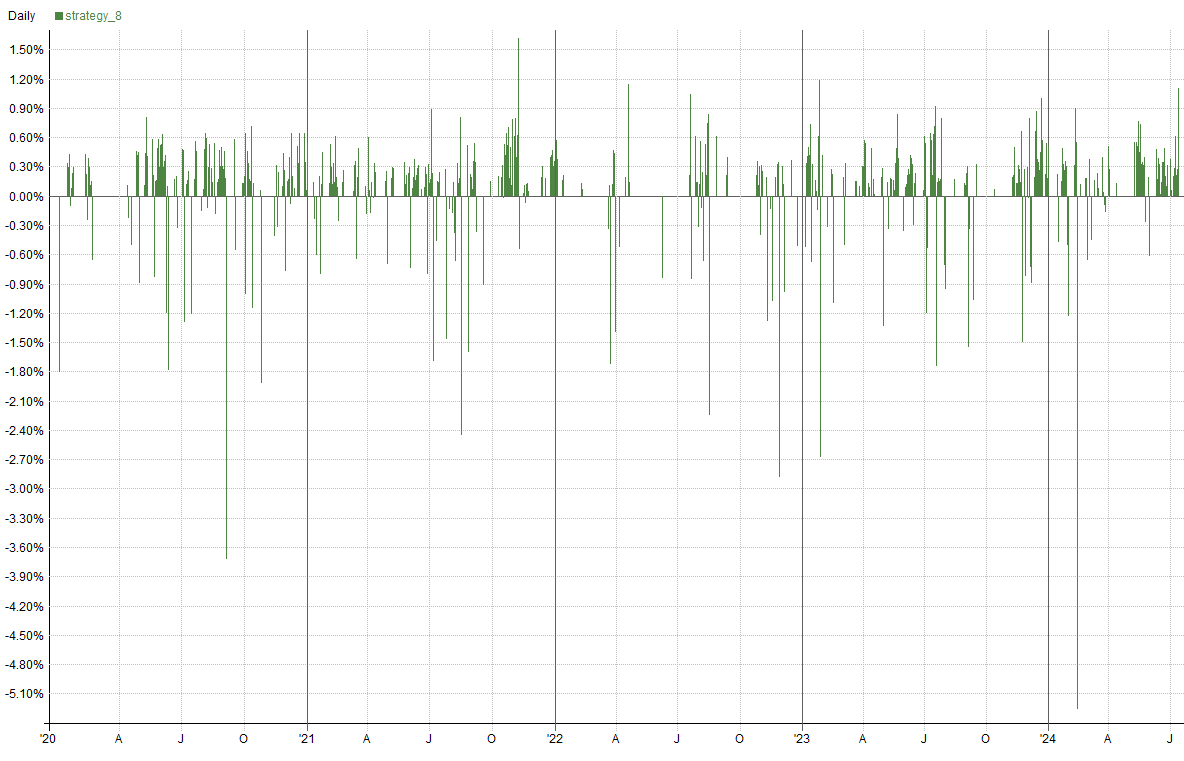
Daily Returns
Monthly Returns

Individual Gains

Monte Carlo — Equity

Monte Carlo — Drawdown

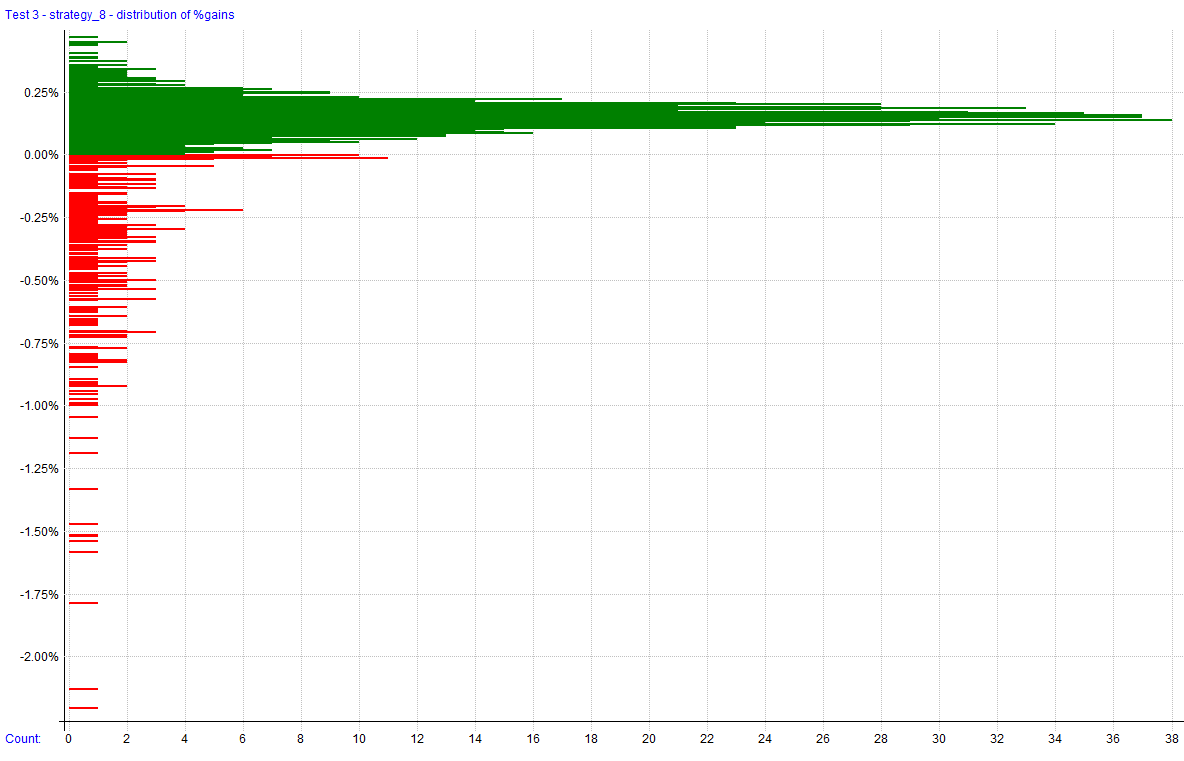
Distribution of Gains
Distribution of Excursions

Strategy 8
This strategy is designed to capture momentum opportunities in futures markets by utilizing short-term RSI signals and a volatility normalized MACD. It also uses a normalized market breadth filter created using the S&P 500 constituents (current and past). It focuses on intraday trading, entering trades on the open and exiting at the close. It started as an experiment to see if the logic from Strategy 7 (a mean reversion strategy) could be reversed and applied successfully. It trades long-side only.
The rest of this post is for paid subscribers. Paid subscribers will have access to the private GitHub where all the Hunt Gather Trade code and strategies live. It is continuously being worked on and will expand as we explore the world of automated trade systems.